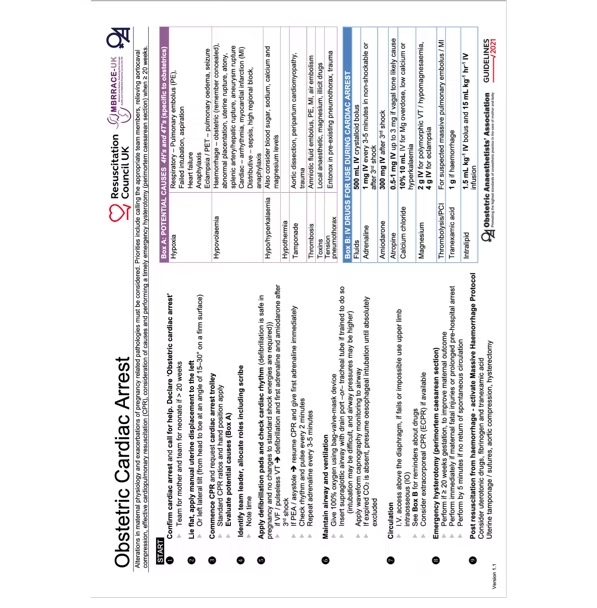
Overview
Resuscitative hysterotomy (also termed perimortem caesarean delivery) is a time-critical intervention performed during maternal cardiac arrest in the second half of pregnancy.
Its primary purpose is maternal resuscitation, not fetal salvage.
Relief of aortocaval compression by emptying the gravid uterus can improve venous return and cardiac output by approximately 20–30%, thereby increasing the likelihood of return of spontaneous circulation (ROSC). A secondary benefit is potential neonatal survival.
Within HALO practice, this is a rare, high-acuity, low-frequency procedure requiring decisive action under extreme time pressure.
- High Acuity – failure results in maternal and fetal death
- Low Occurrence – rarely performed in modern practice
- Time Critical – decision-to-incision delay kills
- Skill Dependent – team skill and speed are essential
Learning Objectives
After completing this module, participants should be able to:
- Explain the physiologic rationale for resuscitative hysterotomy.
- Identify clear indications and timing thresholds.
- Perform a vertical midline resuscitative hysterotomy within the 4–5 minute window.
- Coordinate simultaneous maternal and neonatal resuscitation.
- Manage post-delivery hemorrhage and uterine atony.
Physiologic Rationale
During pregnancy:
- Cardiac output increases up to 50%.
- Systemic vascular resistance decreases under the influence of pregnancy hormones
- Oxygen requirement increases.
- Functional residual capacity decreases.
- Diaphragm is elevated and lung volume reduces.
- Can progress to respiratory failure quickly.
- The gravid uterus compresses the inferior vena cava and aorta
- Prone to supine hypotension and reduced cardiac output
- Mucosal oedema and congestion makes intubation challenging and difficulties in airway management
From approximately 20 weeks gestation (uterus at or above the umbilicus), aortocaval compression significantly impairs venous return.
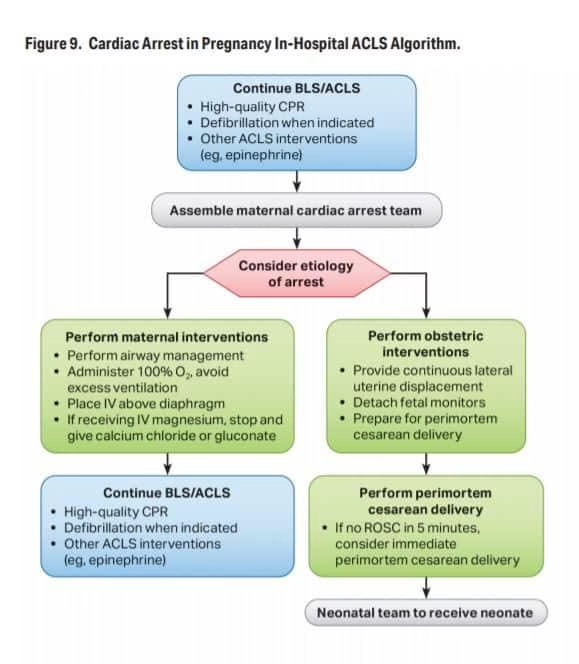
In maternal cardiac arrest:
- Manual left uterine displacement may partially relieve compression.
- Definitive relief occurs only after uterine evacuation.
- Neurologic injury begins within 4–6 minutes of anoxia.
- Maternal and fetal survival decline steeply after 5 minutes without delivery.
The “4-minute rule” therefore guides action:
- Decision at 4 minutes
- Delivery by 5 minutes
Indications
Resuscitative hysterotomy is indicated when:
- Maternal cardiac arrest occurs
- Gestation ≥20 weeks (uterus at or above umbilicus)
- No ROSC after 4 minutes of effective ACLS with uterine displacement
Clinical estimation of gestation:
| Landmark | Approximate Gestation |
| Pubic symphysis | 12 weeks |
| Umbilicus | 20 weeks |
| Xiphisternum | 36 weeks |
If in doubt and the uterus is clearly gravid — proceed with resuscitative hysterotomy.
Contraindications
There are no absolute contraindications in a pulseless patient. As in all resuscitative procedures ensure the environment is safe and a sufficiently skilled clinician is performing the procedure.
In gestations less than 20 weeks emptying the uterus does not offer any benefit to resuscitation and hence not indicated.
If ACLS has resulted in ROSC within 5 minutes , resuscitative hysterotomy is not indicated.
In HALO doctrine: hesitation is the greatest risk.
Causes of Maternal Cardiac Arrest
4H
- Hypoxia( airway obstruction,respiratory failure)
- Hypovolaemia, low blood or fluid volume (severe bleeding, dehydration, burns)
- Hypo/Hyperkalemia ( also include acidosis)
- Hypothermia
4T
- Tension pneumothorax
- Tamponade
- Toxins( drug overdosage, anaphylaxis, poisonous substances)
- Thrombosis
Incidence is rare (approximately 1 in 30,000 pregnancies), reinforcing the HALO principle: train for the uncommon.
Equipment
Minimal equipment is required. Do not delay for a full obstetric tray. Use a thoracotomy set if available.
Essential equipment.
- Scalpel (#10 or #20 blade)
- Heavy scissors
- Cord clamps (or artery clamps)
- Gauze
- Suction (if available)
- Uterotonics (oxytocin preferred)
Neonatal resuscitation equipment should be immediately available. Designate a separate space for neonatal resuscitation so that the teams can work in tandem but without distraction.
Team Structure
Resuscitative hysterotomy is performed at the site of arrest.
Roles:
- Team leader (ALS coordination)
- Proceduralist (most surgically experienced clinician present- most likely candidate will be Emergency Medicine Physician)
- Airway lead
- CPR provider
- Medication nurse
- Neonatal resuscitation team
Do not transfer to theatre.
Procedure
Maternal CPR continues throughout.
Step 1 – Continue Modified ALS
- Supine position
- Manual left uterine displacement
- High-quality chest compressions
- Early airway control

Step 2 – Rapid Abdominal Access
- Clean abdomen with antiseptic preparation
- Make a vertical midline incision from pubic symphysis to above the level of uterus.
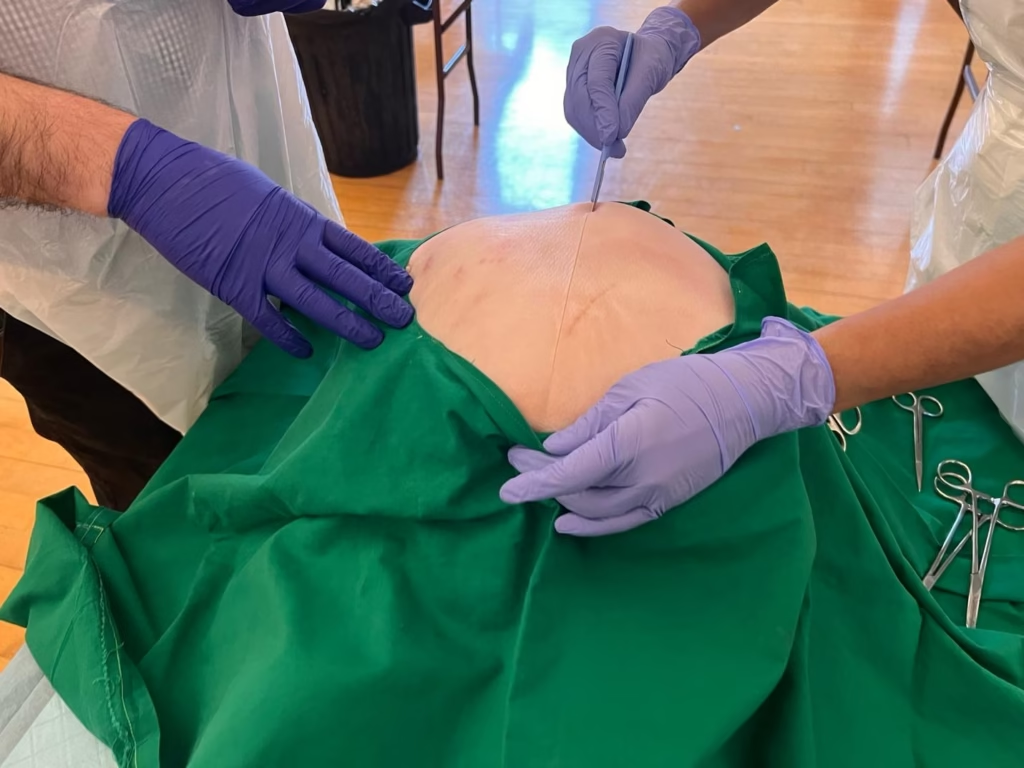
- Incise skin, subcutaneous tissue, linea alba, and peritoneum.
- Retract abdominal wall, Expose uterus.

Midline incision minimizes bleeding and maximizes speed.
Step 3 – Uterine Incision
- Incise lower uterine segment vertically (~3–5 cm).
- Extend incision superiorly with scissors.
- Enter amniotic cavity.
- Deliver the fetus manually.

- Clamp and cut cord.
- Transfer neonate immediately.
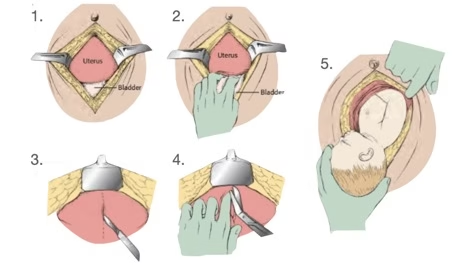
Courtesy: LITFL

Time from skin incision to delivery should ideally be under 1 minute.
Step 4 – Post-Delivery Actions
- Deliver placenta.
- Manually sweep the uterine cavity.
- Administer oxytocin 5 IU IV (if ROSC achieved).
- Uterine massage.
- Pack the abdominal cavity with large swabs.
- Continue maternal resuscitation.
If ROSC achieved:
- Control hemorrhage
- Consider TXA
- Antibiotic prophylaxis
- Prepare for definitive surgical management- transfer patient to emergency theatre for wound exploration and closure.
Complications
Maternal:
- Hemorrhage
- Uterine atony
- Bladder or bowel injury
- Thromboembolism
- Infection
Neonatal:
- Hypoxic injury
- Extraction trauma
Complications increase significantly with delayed decision-making.
Neonatal Considerations
Fetal survival is influenced by:
- Arrest-to-delivery time
- Gestational age (>24–25 weeks better outcomes)
- Quality of CPR
- Availability of neonatal intensive care
- Pre-arrest maternal physiology
Survival has occurred beyond 5 minutes, but probability declines rapidly after 10–15 minutes.
Post-Procedure Management
If maternal ROSC:
- Ongoing hemorrhage control
- Monitor coagulopathy
- ICU admission
- Multidisciplinary coordination
If no ROSC:
- Continue ALS per institutional protocol
- Document timing clearly
Remember to debrief
HALO Performance Principles
Resuscitative hysterotomy is fundamentally a decision procedure.
Common barriers:
- Waiting for obstetrics
- Waiting for ultrasound
- Waiting for sterility
- Waiting for confirmation of gestation
None are required.
The most difficult step is making the decision for the procedure in 4 minutes.
Key Takeaways
- Primary goal: improve maternal survival.
- Indicated at ≥20 weeks gestation.
- Decide in 4 minutes.
- Deliver by 5 minutes.
- Perform in a resuscitation room.
- Continue CPR throughout.
- Do not delay.
Appendix 1
Example scenario
Scenario: 32-week pregnant patient in arrest from amniotic fluid embolism.
Performance metrics:
- Decision announced by 4 minutes
- Skin incision by 4:30
- Delivery by 5:00
- Continuous CPR maintained
- Neonatal resuscitation initiated within 60 seconds of delivery
Appendix 2